
Story at-a-glance
- Within weeks of the pandemic outbreak, it had become apparent that the standard practice of putting COVID-19 patients on mechanical ventilation was a death sentence; 76.4% of COVID-19 patients (aged 18 to 65) in New York City who were placed on ventilators died. Among patients over age 65 who were vented, the mortality rate was 97.2%
- The recommendation to place COVID patients on mechanical ventilation as a first-line response came from the World Health Organization, which allegedly based its guidance on experiences and recommendations from doctors in China. But venting COVID patients wasn’t recommended because it increased survival. It was to protect health care workers by isolating the virus inside the vent machine
- Data suggest around 10,000 patients died with COVID in NYC hospitals after being put on ventilators in spring 2020. Other metropolitan areas also saw massive spikes in deaths among younger individuals who were at low risk of dying from COVID. It’s possible many of these deaths were the result of being placed on mechanical ventilation
- The WHO must be held accountable for its unethical recommendation to sacrifice suspected COVID patients by using ventilation as an infection mitigation strategy — especially considering they’re now trying to get unilateral power and authority to make pandemic decisions without local input
- Showing how the WHO’s recommendation to put patients on mechanical ventilation resulted in needless death among people who weren’t at great risk of dying from COVID is perhaps one of the most powerful talking points a country can use to argue for independence and rejection of the WHO’s pandemic treaty
Within weeks of the pandemic outbreak, it had become apparent that the standard practice of putting COVID-19 patients on mechanical ventilation was a death sentence.1
By early April 2020, many doctors were already questioning their use, as data2 showed 76.4% of COVID-19 patients (aged 18 to 65) in New York City who were placed on ventilators died. Among patients over age 65 who were vented, the mortality rate was a whopping 97.2%.
If you were older than 65, you were 26 times more likely to survive if you were NOT placed on a vent.3 A small study from Wuhan, China, put the ratio of deaths at 86%,4 and in Texas, 84.9% of patients died after more than 96 hours on a ventilator.5
In a widely-shared YouTube video6 (above) posted March 31, 2020, Dr. Cameron Kyle-Sidell, a critical care specialist at the Mount Sinai Health System in New York, warned that “we must change what we are doing if we want to save as many lives as possible.” Sidell was adamant that doctors were “treating the wrong disease” and that putting COVID patients on mechanical ventilation was all wrong.
[…]
Why Were COVID Patients Put on Vents?
The recommendation to place COVID patients on mechanical ventilation as a first-line response came from the World Health Organization,7 which in early March 2020 published a COVID-19 provider guidance8 document to health care workers, based on experiences and recommendations from doctors in China.
According to the WHO, treatment needed to be rapidly escalated to mechanical ventilation. Ideally, patients should be placed on it immediately.9 What escaped the public was the primary reason why. Venting COVID patients wasn’t recommended because it increased survival; rather, it was to protect health care workers by isolating the virus inside the mechanical vent machine.
Using less invasive positive air pressure machines could result in the spread of infectious aerosols, the WHO warned. In other words, they put patients to death to “save” staff and other, presumably non-COVID, patients.
[…]
Even Dr. Anthony Fauci, in a mid-June 2022 lecture (above), admitted that placing patients on mechanical ventilation did more harm than good.
[…]
Yet government treatment guidelines, to this day, include invasive mechanical ventilation.12 If the White House Coronavirus Task Force knew in the summer of 2022 that venting patients caused more harm than good, why didn’t they instruct hospitals to stop using it? Or at bare minimum, strongly advise against it?
And why did the government continue to financially incentivize the use of mechanical ventilation after they’d realized how bad it was? While many hospitals did cut down on their use of mechanical ventilation toward the end of 2020 and beyond, it still hasn’t been entirely replaced with noninvasive strategies shown to be far more effective.13
Many ‘COVID Patients’ Didn’t Have COVID
The matter becomes even more perverse when you consider that many “COVID cases” were patients who merely tested positive using faulty PCR testing. They didn’t have COVID but were vented anyway, thanks to the baseless theory that you could have COVID-19 and be infectious without symptoms.
Hospitals also received massive financial incentives to diagnose patients with COVID — whether they had it or not — and to put them on a vent. They also received bonuses for using toxic remdesivir, and they were paid for each COVID death as well. The entire system was set up to reward hospitals for misdiagnosing, mistreating and ultimately killing patients.
China also benefited from the WHO’s misguided advice. While the U.S. clamored for more ventilators, Chinese hospitals started relying on them less and instead they were being exported in huge quantities.14
How Many COVID Patients Were Killed by WHO’s Bad Advice?
Just how many COVID-19 patients were killed by being placed on mechanical ventilation in the spring of 2020? That’s a question attorney and author Michael P. Senger tries to answer in his May 25, 2023, article “The Great COVID Ventilator Death Coverup.”15
[…]
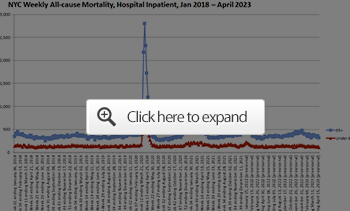
Inpatient Mortality Around the US, 2020 Through Present
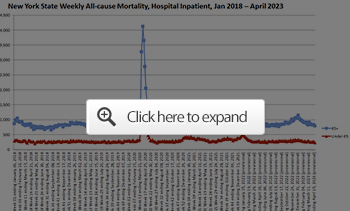
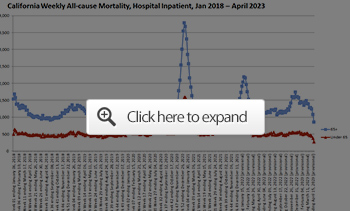
Senger goes on to show the same all-cause mortality graphs for hospital inpatients for each of the largest cities in the U.S.: Chicago, Dallas, Houston, Los Angeles and Washington, D.C. All show massive spikes in hospital deaths, especially among the elderly (65 and older), around the same time periods as NYC. He also produced charts for deaths on the state level, as follow:20


A Morally Indefensible Coverup
Senger points out that, in speaking with other attorneys, most agree that hospitals face virtually no risk of litigation over ventilator deaths, for the simple reason that everyone perceived COVID to be a global emergency, and during emergencies, you just do the best you can with what you have and what you know.
[…]
Even so, “the situation is morally inexcusable,” Senger says, adding that we do need to get to the bottom of how and why these patients died. I agree. While Senger wants the truth to understand what happened and to honor the diseased, I would add that we need the truth in order to avoid making the same mistake again, because there will be a next time.
The WHO Must Be Held to Account
The WHO must be held accountable for its unethical recommendation to sacrifice suspected COVID patients by using ventilation as an infection mitigation strategy — especially considering they’re now trying to get unilateral power and authority to make pandemic decisions without local input.
Showing how the WHO’s recommendation to put patients on mechanical ventilation resulted in needless death among people who weren’t at great risk of dying from COVID is perhaps one of the most powerful talking points a country can use to argue for independence and rejection of the WHO’s pandemic treaty.
They simply cannot be trusted to make sound medical decisions for the whole world. No one is. We need to allow local medical experts to make the calls in situations like this, and to collaborate and share information between themselves. The top-down one-size-fits-all medical paradigm that the WHO wants to implement is nothing short of disastrous, and the COVID pandemic response proves it.
Also, let’s not forget that the misuse of mechanical ventilation created the appearance that COVID was exceptionally deadly, regardless of your age, which in turn helped promote acceptance of the experimental COVID shots that are now a leading cause of frequent sickness, chronic disability and excess deaths. Of course, that’s also being covered up.
In the final analysis, the WHO’s handling of the COVID pandemic will undoubtedly go down as the worst in medical history. Can we really trust them to make better decisions in the future?
I think not, which is why we must do everything in our power to prevent the U.S. from signing the pandemic treaty. Better yet, we need to exit the WHO entirely. To that end, I urge you to contact your local House representatives and Senators and urge them to:
- Support the No WHO Pandemic Preparedness Treaty Without Senate Approval Act24,25,26,27,28
- Withhold funding for the WHO
- Support U.S. withdrawal from the WHO
[…]

Pingback: Mass Murder at the Hospital | Aisle C
lessee now. im the head of a hospital and the first 9 out of 10 ventilated patients die. wouldnt i deduce that ventilating was not just ineffective but deadly? shameful. these doctors that continued the treatment after the effect became obvious are monsters. but of course they were just following orders. orders of the WHO. the WHO instigated mass murder. it would be wise to at least be aware of that. because all signs indicate they are planning to do it again. and we need to recognize it as genocide and that WHO is (has become?) a genocidal institution.
LikeLike
I think the doctors at the beginning could have been forgiven – given that the Covid mortality in China (one of the first affected countries) was 15%. But I see no excuse for blindly following the WHO after August 2020, when it became apparently that mortality in Europe and the US was closer to 1% (same as the common flu).
LikeLike
absolutely. but hey, they were getting paid.
LikeLiked by 1 person
My husband was admitted to a local hospital with Covid – pneumonia in January 2022. In less than 2 weeks he was ventilator dependent with induced coma. In 2 weeks he had MERSA. Soon after that he had multiple organ failure,flaccid generalized paralysis, severe lung damage, and rectal bleeding.Required multiple blood transfusions. He gave up and asked me to get him disconnected after 68 days of suffering. Unfortunately other people I know went throughout same protocol with the same sad end.
LikeLike
From what I’ve been reading, Maria, in many cases the pneumonia wasn’t caused by Covid but by a secondary bacterial infection, which could have been treated with an antibiotic. This is blatant malpractice – putting people on respirators to protect staff instead of offering appropriate treatment.
Really sorry to hear what they put you and your husband through. Thanks for your comment.
LikeLike