

Peter C Goetzsch
I dedicate this article to all women invited to mammography screening and those who love them because the public has consistently been lied to, for over 40 years. In invitations to screening, women have been told that by detecting cancers early, screening saves lives and leads to less invasive surgery.1,2 I shall demonstrate that all three statements are wrong.
Women are still being told these lies, by professional associations, screening advocates, screening researchers, cancer charities, and national boards of health.3-5 The American Cancer Society declares in a headline that “Mammography Saves Lives”4 and claims, with no references, that results from many decades of research clearly show that women who have regular mammograms are less likely to need aggressive treatments like surgery to remove the entire breast (mastectomy).5
Screening Does Not Save Lives
In the randomised trials of mammography screening, the risk ratio for overall mortality after 13 years of follow-up was 0.99 (95% confidence interval 0.93 to 1.03) for those trials with adequate randomisation.6 The estimate happened to be the same for the other trials, some of which were so poorly randomised that the average age in the two compared groups was not the same, which makes an analysis of overall mortality unreliable.
For two of the three adequately randomised trials, those from Canada and the UK, there are follow-up data after 25 and 23 years, respectively.7,8 The risk ratio for overall mortality was 1.01 (95% confidence interval 0.98 to 1.03) for all three trials (both with a fixed effect and a random effects model, Comprehensive Meta Analysis Version 3.0). In the table, the year means the year the trial started:
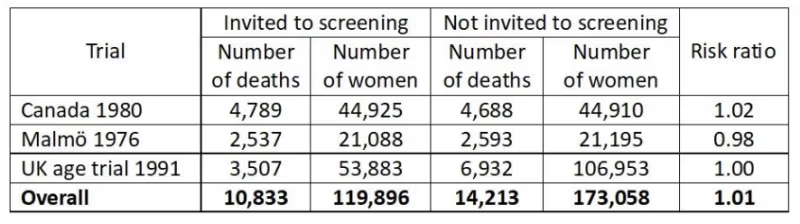
This is a very strong result as it is derived from a total of 25,046 deaths. We can therefore say with great confidence that mammography screening does not save lives.
If we restrict the analysis to the two trials with a very long follow-up, the result is the same, a risk ratio of 1.01 (0.99 to 1.04).
Breast Cancer Mortality Is a Seriously Flawed Outcome
It will surprise most people to learn that we cannot trust what has been reported in the randomised trials about the effect of screening on breast cancer mortality but this is an objective fact.6
A minority of the women who died were autopsied, and in several trials, cause of death was not assessed blindly.6 I have documented that assessment of cause of death was seriously biased.6,9 If we include all trials in the analysis, we would expect to see the greatest reduction in breast cancer mortality in those trials that were most effective in lowering the rate of node-positive cancers (cancers that had metastasised) in the screened group.
This was indeed the case, but the regression line was in the wrong place. It predicts that a screening effectiveness of zero (i.e. the rate of node-positive cancers is the same in the screened groups as in the control groups) results in a 16% reduction in breast cancer mortality (95% confidence interval 9% to 23% reduction).6,9 This can only happen if there is bias, and further analyses showed that assessment of cause of death and of the number of cancers in advanced stages were both biased in favour of screening.
Systematic reviews that include all the trials, also the poorly randomised ones, have reported that mammography screening reduces breast cancer mortality by 16-19%.6,10 As this estimate is of the same size as the bias in the regression analysis, this suggests that screening does not lower breast cancer mortality.
Another reason why breast cancer mortality is a flawed outcome is that screening leads to overdiagnosis, which is the detection of cancers and precursors to cancer (carcinoma in situ), which would not have come to the attention of the woman in her remaining lifetime and therefore would not have become a problem without screening. Since it is not possible to distinguish between harmless cancers and dangerous ones, they are all treated, and radiotherapy and chemotherapy given to women who are healthy increase their mortality.6
If we take into account the cardiac and lung cancer deaths caused by the type of radiotherapy used when the screening trials were carried out and generously assume that screening reduces breast cancer mortality by 20% and results in only 20% overdiagnosis of healthy women, then there is no mortality benefit from screening.11
Finally, it is noteworthy that the most unreliable trials were those that reported the greatest reductions in breast cancer mortality.6 The difference in the effect estimates between the adequately randomised trials and the poorly conducted trials was statistically significant, both after 7 and 14 years of follow-up (P = 0.005 and P = 0.02, respectively).12
Total Cancer Mortality
Since misclassification of cause of death often concerns deaths from other cancers,6 total cancer mortality is a less biased outcome than breast cancer mortality.
Some trialists have not reported what the total cancer mortality was but we have data from the three adequately randomised trials.6,8 There was no effect of screening on total cancer mortality, including breast cancer, risk ratio 1.00, 95% confidence interval 0.96 to 1.04. There were two different age groups in the Canadian trial, 40-49 (a) and 50-59 years (b):
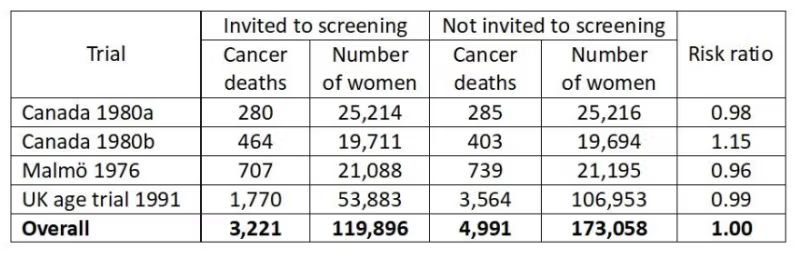
Since total cancer mortality is less biased than breast cancer mortality, it is of interest to see what the expected cancer mortality (including breast cancer mortality) would have been if the reported reduction in breast cancer mortality of 29% after 7 years in the poorly randomised trials6 were true.
It would have been a risk ratio of 0.95, which is significantly lower (P = 0.02)6 than what was actually found. This provides further evidence that assessment of cause of death was biased in favour of screening.
Breast Cancer Is Not Detected Early but Very Late
If we assume that the observed doubling times in longitudinal tumour studies are constant from initiation till the tumour becomes detectable, the average woman has harboured the cancer for 21 years before it acquires a size of 10 mm and becomes detectable on a mammogram.13
Given this large time span, it is misleading to call it “early detection” also because the effect of screening is trivial, namely to advance the diagnosis by less than a year.13
Yet all authorities repeat this mantra. As it is impossible that everyone working with cancer is unaware of the basics of tumour biology, we can draw the conclusion that the public all over the world is being misinformed. This is fraud because it is deliberate and because women think “early detection” will save their lives.
I once asked a famous tumour biologist, Keld Danø, during a coffee break at an international meeting, whether he agreed with me that it was impossible to lower breast cancer mortality by 30% with screening, based on our knowledge of tumour biology.14 He agreed. When I asked why people like him didn’t participate in the scientific debate, he didn’t reply and it is not difficult to imagine why. It is not wise to point out that your colleagues are wrong when you are on the receiving end of major funds from a cancer charity that touts screening.
The women suffer while everyone else prospers.
The earliest cell changes, carcinoma in situ, are not detected unless the women get a mammogram. In our systematic review of countries with organised screening programmes, we found an overdiagnosis of 35% for invasive cancer and 52% when we included carcinoma in situ.15
Although less than half of carcinoma in situ cases progress to invasive cancer,16,17 the women are nevertheless routinely treated with surgery, drugs, and radiotherapy.
The deep irony is that the surgery is often mastectomy because the cell changes may be diffusely spread in the breast, and sometimes even in both breasts. In New South Wales, one-third of women with carcinoma in situ had a mastectomy,18 and in the UK, carcinoma in situ was more often treated by mastectomy than invasive cancer,19 and the number of women treated by mastectomy almost doubled from 1998 to 2008.20
This brings us to the third big falsehood in the propaganda about mammography screening.
Screening Does Not Decrease but Increases Mastectomies
Because of the substantial overdiagnosis of invasive cancer and carcinoma in situ, and because screening only advances detection of invasive cancers slightly,13 it is inevitable that screening increases mastectomies.
In the randomised trials of screening, we found 31% more mastectomies in the screened groups than in the control groups.6
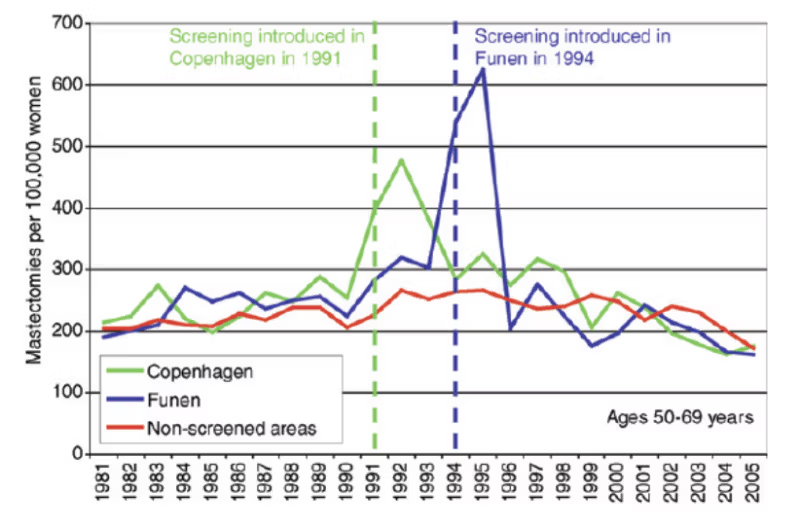
Denmark is a unique country to study this in practice as we had a period of 17 years (1991-2007) where only about 20% of potentially eligible women were invited to screening because some counties did not have screening.21 When screening starts, more breast cancer diagnoses than usual will be made and there will be more mastectomies. However, as can be seen on the graphs, the huge increases in mastectomies are not compensated by a drop in mastectomies later where there was a similar decline in mastectomies in non-screened areas as in screened areas:22
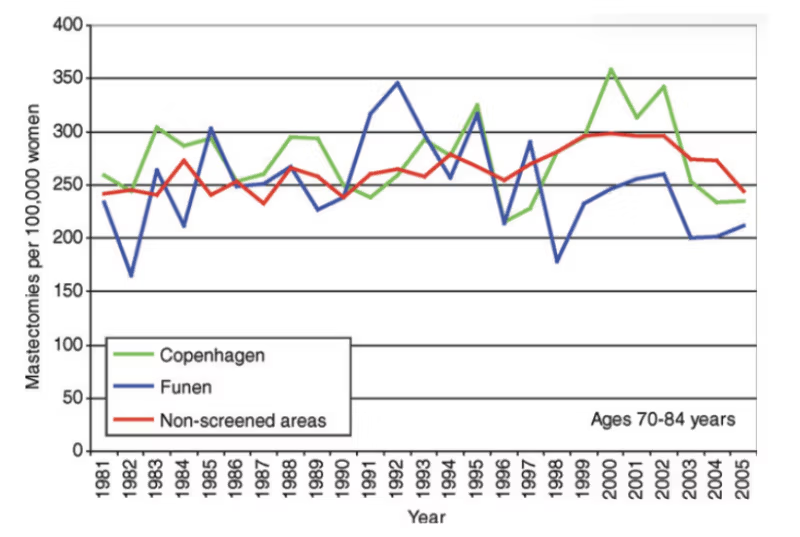
Moreover, as the next graph shows, there is no compensatory drop in old age groups:22
Yet women are told that screening leads to less invasive surgery, with fewer mastectomies. This is disinformation in the extreme.
The most commonly used trick used to disinform the women about this issue is to report percentages instead of numbers.3 Imagine a town with a certain level of crime. You divide the crimes into serious and less serious ones. Over a period of time, the rate of serious crime increases by 20% and the rate of less serious crime by 40%. This is a development for the worse. But although more people are exposed to serious crime and more people are exposed to less serious crime as well, a trickster would say that, as there are now relatively fewer cases of serious crime, the situation has improved.
It is deplorable that people who know better – screening researchers, cancer charities, national boards of health, etc – have lied to the public this way3 and still do, in direct contrast to logic and the scientific evidence.
I dryly remarked in my book that if they continued their line of research for other diseases, they may find the recipe for eternal life.3 I also noted that the problem with lying is that
sooner or later people usually contradict themselves, which they did in relation to a study they had published in The Lancet.3
A common way of duping the readers is to say that early detection of breast cancer “reduces mortality”34 without specifying what kind of mortality this is, which makes the reader believe that screening saves lives.
The most common error in the screening literature could be that people falsely translate a recorded effect on mortality from a cancer into an effect on all-cause mortality. We see claims everywhere that common cancer screening tests save lives but a systematic review of the randomised trials found that the only screening test with a significant lifetime gain was sigmoidoscopy. It extended life by 110 days on average, and as the 95% confidence interval went from 0 to 274 days, this result was on the verge of not being statistically significant.35
Another common trick is to use hypothetical statements when we have certain knowledge. For example, authors may write – even in our most esteemed medical journals – that overdetection “may” occur for invasive cancers and that it “may” cause harm through unnecessary labelling and treatment of patients who, without screening, “might” never have been diagnosed.34 These are not hypothetical possibilities; they are inevitable consequences of screening.
[…]
Via https://brownstone.org/articles/the-three-big-lies-about-mammography-screening/
