I have blogged previously (see Menopause: Made in the USA) about the negative effects of the “corporatization” of health care in the US. “Disease mongering” is a particularly nasty one. This occurs when pharmaceutical companies “medicalize” common conditions in order to market drugs that supposedly treat them.
Thanks to skillful marketing, Eli Lilly has turned premenstrual syndrome (PMS) into a profit-making commodity nearly as lucrative as menopause and “childhood bipolar disorder” (see Drug Companies: Killing Kids for Profit).
In 1994, the American Psychiatric Association (APA) included premenstrual dysphoric disorder (PMDD) in their diagnostic manual “as a possible mental disorder requiring more research.” They have continued the diagnosis in DSM V. Although DSM IV lists PMDD as a strictly “research” diagnosis, Eli Lilly immediately seized on it as a genuine disorder and devised a marketing strategy to profit from it.
The Difference Between PMS and PMDD
Approximately 80-90% of women worldwide report physical and emotional changes in the 7-10 days prior to the onset of menstruation. For most women, these consist of minor physical changes similar to those of early pregnancy (water retention, breast swelling and tenderness and abdominal bloating).
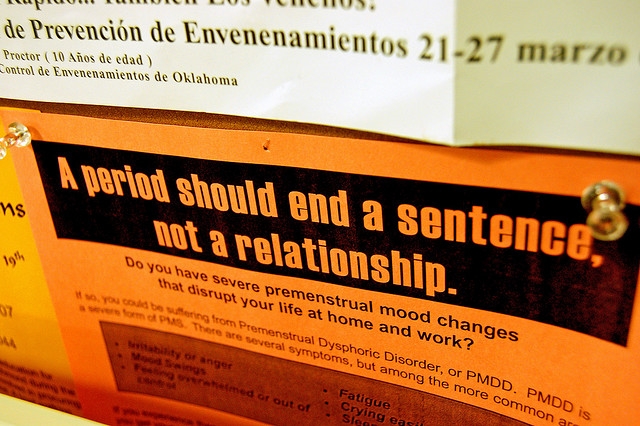
Approximately 1/3 of women note mental and emotional changes (aka PMS) – depression, anxiety, fatigue, irritability, insomnia, difficulty concentrating – that have a minor impact on their daily functioning.
Although the APA has yet to agree PMDD even exists as a disorder, there are numerous claims in psychiatric and women’s health literature that approximately 3-8% of women suffer from it. By definition, a woman can only qualify for a PMDD diagnosis if they experience a “marked” decrease in normal functioning due to premenstrual mood changes. A rigorous Swedish study ascertained that the true percentage of women experiencing a “marked” decrease in functioning before their period closer to 1.3%.
A Golden Marketing Opportunity for Eli Lilly
Once the patent on a drug expires, other manufacturers are free to produce cheaper generic versions, resulting in plummeting sales of the original brand name drug. In 1999 Lilly, facing the expiration of its patent on Prozac, exploited the new “diagnosis” of PMDD by re-branding Prozac as a feminine pink and purple tablet called Sarafem.
In 2001, the FDA approved Sarafem for “PMDD,” on the basis of double blind studies involving several hundred women. Lilly reported a 60% response rate in women who took it for five cycles, with greater effectiveness in women who took it continuously throughout the month (as opposed to 7-10 days before their period).
Hopefully psychiatrists aren’t quite so gullible as the FDA, given Prozac’s limited effectiveness in treating depression. Thirty years of double blind studies reveal that depressed patients who take Prozac have an average response rate of 38-40%. In fact, statistical analysis of all randomized controlled trials reveal that all SSRI’s (i.e. Prozac, Zoloft, Paxil, citalopram, etc) are only slightly more effective than a placebos, which works 33-37% of the time.
Skillful Marketing Adds Billions to US Health Care Bill
Charging three dollars per dose for their pink and purple Sarafem tablets (in contrast to 41 cents per dose for generic fluoxetine), Lilly launched a massive marketing campaign to convince women they suffered from PMDD. In 2001, the year Serafem came out, nearly 100,000 prescriptions were sold, reaping Lilly $85 million in profits.
Given the soaring cost of health care in the US (the main reason millions of Americans go without medical care), it strikes me as unethical and immoral to trick doctors and women into wasting nearly a billion dollars on pink and purple pills with a fancy name, when generic fluoxetine would have been equally effective at 1/9 the cost.
Research Evidence for “Natural” Treatments
What I find really fascinating about the PMS/PMDD controversy is that it’s one of the few women’s health “conditions” in which there are more double blind placebo trials of “alternative” or “natural” treatments than medication trials. The three “alternative” treatments that have shown clear effectiveness in randomized controlled trials are omega 3 supplements, Vitamin D and the chaste tree berry or chasteberry. In fact, much of this research suggests that PMS-related mood changes may actually represent a nutritional deficiency of omega 3 and/or Vitamin D.
Omega 3 oil is the most studied in PMS-related mood changes, largely owing to its proven efficacy in depression and large cross cultural studies revealing that populations (for example Asians and Norwegians) consuming large amounts of fish (a primary source of omega 3) in their diets have an extremely low incidence of depression.
Vitamin D, has also proved helpful for depression in double blind studies, especially in elderly depressives suffering from documented Vitamin D deficiency. Other studies show that 1,000 – 2,000 international units of Vitamin D is helpful in alleviating premenstrual symptoms.
This finding correlates with an extremely low incidence of PMS in Asian women. The same oily fish that are a rich source of omega 3 are the only natural food source of Vitamin D (the majority of us derive Vitamin D from exposure to sunlight).
Three double blind studies in the British Medical Journal, the Archives of Gynecology and Obstetrics and the Journal of Women’s Health and Gender-based Medicine reveal that chasteberry helps approximately 52% of women with PMS. Chasteberry is an herbal remedy used by Hippocrates in ancient Greece for pre-menstrual symptoms. It’s believed to work by lowering prolactin (a pituitary hormone influencing milk production). High prolactin levels are a recognized, but infrequent, cause of depression.
Take Home Message: Try Natural Remedies First
In light of all the above studies, common sense would dictate that women who suffer from PMS should try a combination of omega 3 and 1,000-2,000 IU of Vitamin D for a minimum of six months before resorting to either Sarafem or generic fluoxetine. Both have potentially serious long term side effects. Owing to their effect on serotonin receptors in the brain, SSRI’s can be very difficult to stop. Moreover they are associated with a loss of bone density, which increases the risk of osteoporosis and hip fracture in later life, and possibly linked to breast and ovarian cancer
photo credit: taberandrew via photopin cc